MEET THE SURGEON

Dr. Michael William Kessler, MD, MPH, FAOA
-
-
-
-
- Chief, Department of Orthopaedic Surgery, Division of Hand Surgery,
MedStar Orthopaedic Institute, Washington, DC
- Chief, Department of Orthopaedic Surgery, Division of Hand Surgery,
-
-
-
DISCLAIMER
The opinions expressed by Dr. Kessler are those of Dr. Kessler and not necessarily those of Field Orthopaedics. Individual experiences may vary.
The procedure described in the report may differ from the manufacturer’s surgical technique. Surgeons are advised to review the product specific surgical technique prior to performing any surgery.
A surgeon must always rely on their own professional clinical judgement when deciding whether to use a particular product when treating a particular patient. A surgeon must always refer to the instructions for use, product label and surgical technique before using any Field Orthopaedics product. Product may not be available in all markets. Please contact your Field Orthopaedics representative if you have any questions about availability of Field Orthopaedics products in your area.
OVERVIEW
A 20-year-old male sustained a displaced right first metacarpal fracture after a fall, presenting with significant pain, limited thumb motion, and angular deformity. Radiographs confirmed the displaced fracture. He underwent open reduction and internal fixation (ORIF) with a 3.5 mm x 40mm NX Nail intramedullary nail. The procedure achieved stable fixation and corrected alignment. Postoperatively, the patient experienced excellent recovery, with resolution of pain and return of full digital flexion by five weeks, at which point he was cleared to return to work. Follow-up confirmed stable hardware and fracture healing with a good prognosis for full function.
CASE INTRODUCTION
A 20-year-old male sustained a displaced right first metacarpal fracture following a ground-level fall while walking home. He was initially evaluated in an emergency department, where radiographs confirmed the injury, and a splint was applied. Upon presentation, the patient reported moderate to severe pain, and examination revealed significant angular deformity of the thumb metacarpal that would have limited motion and function if left untreated. Given these findings and the patient’s interest in surgical correction, open reduction and internal fixation (ORIF) was recommended. The procedure, along with associated risks, benefits, and postoperative care, was thoroughly discussed.
CASE PRESENTATION
On examination, the patient was alert, oriented, and in no acute distress. There was maximal tenderness and limited range of motion of the right thumb due to pain, but intact Anterior Interosseous Nerve (AIN), Posterior Interosseous Nerve (PIN), and ulnar nerve function, with normal capillary refill and sensation in the median, radial, and ulnar nerve distributions.
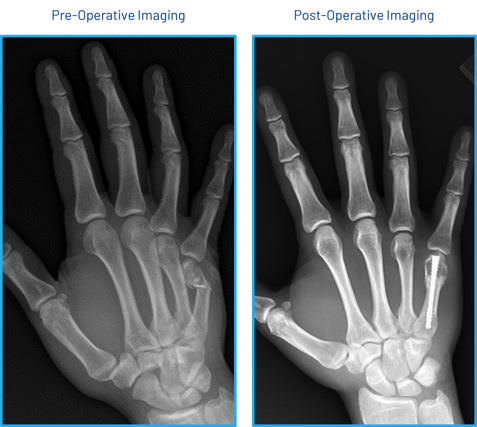
Radiographs reviewed confirmed a displaced fracture of the right first metacarpal. After discussing treatment options, including both conservative and surgical management, the patient elected to proceed with ORIF.
Below: Pre-Operative Imaging

PRE-OPERATIVE PLAN
The patient underwent surgery 7 days after the injury. The procedure took place under general anesthetic with the patient in supine position.
INTRAOPERATIVE DETAILS
A longitudinal incision was made dorsally over the thumb metacarpophalangeal (MCP) joint. Dissection was carried down through the skin and subcutaneous tissue. The extensor pollicis longus (EPL) and extensor pollicis brevis (EPB) tendons were identified, and the raphe between them was incised, extending distally across the joint. A dorsal capsulectomy was performed to expose the metacarpal head.
The fracture was reduced and a guidewire for a 3.5 mm diameter intramedullary Nail (NX Nail) was then advanced down the shaft of the first metacarpal. Intraoperative fluoroscopy confirmed accurate guidewire placement and satisfactory fracture reduction.
A cannulated drill was passed over the guidewire, followed by intramedullary placement of the 3.5 mm x 40mm NX Nail, achieving stable fixation of the fracture. Fluoroscopy was used throughout to confirm appropriate nail positioning, as well as improvement in length, alignment, and rotational correction of the first metacarpal. With tenodesis testing, no malrotation was observed during wrist flexion and extension.
The wound was irrigated thoroughly. The EPL and EPB tendons were repaired using 4-0 FiberWire sutures in an interrupted horizontal mattress fashion. The skin was closed with 4-0 Monocryl sutures, followed by application of Dermabond and Steri-Strips.
Below: Intra-Operative Imaging

POSTOPERATIVE CARE
The patient was placed into a thumb spica splint immediately postoperatively. The procedure was well tolerated without complications. The patient was advised to follow up for splint removal and initiation of range of motion exercises under the guidance of occupational therapy.
FOLLOW UP
One day review
The patient reported well-controlled pain and some numbness in the right thumb. Examination revealed a well-healed incision, no focal tenderness, full digital flexion to the distal palmar crease, intact sensation in the median, radial, and ulnar nerve distributions, and capillary refill under 2 seconds. X-rays demonstrated appropriate hardware placement, improvement in length, alignment, and rotation of the fracture site, with early signs of generalized disuse osteopenia.
The patient was referred to occupational therapy for a custom splint and instructed on incision care, with clearance to begin gentle washing of the surgical site.
Five week review
The patient was doing well postoperatively with no pain and a desire to return to work. Physical exam showed a well-healed incision without tenderness, full range of digital flexion, normal sensation, and no tenderness at the fracture site. Pain was rated 0/10. The patient was advised to begin weaning from the brace, continue working on range of motion exercises, and was cleared to return to work activities with continued activity modification as needed.
CONCLUSION
In this case, open reduction and internal fixation with an NX Nail provided stable fixation for a displaced fracture of the right first metacarpal shaft in a young, active patient. The construct maintained fracture alignment, improved length and rotational control, and allowed for early mobilization under the guidance of occupational therapy.
Postoperative recovery has been excellent, with no complications, well-controlled pain, and progressive return to function. The patient is cleared to return to work and will continue supervised rehabilitation to optimize range of motion and hand strength. Follow-up imaging confirmed stable hardware position and near-anatomic alignment. The patient’s prognosis for full functional recovery remains very good.
References
1. Field Orthopaedics. (2023). NX Nail Metacarpal Long Surgical Technique. Brisbane, Australia: Field Orthopaedics.
FO-010920-MM Version 1 May 2025